



Comprehensive Medical Guide to Aclasta (Zoledronic Acid)
Aclasta, known generically as zoledronic acid, is a potent third-generation bisphosphonate medication that has revolutionized the treatment of bone metabolism disorders. By inhibiting osteoclast-mediated bone resorption, Aclasta plays a critical role in managing conditions characterized by excessive bone breakdown, such as osteoporosis and Paget’s disease of bone.
This guide provides an in-depth clinical analysis of Aclasta, intended for healthcare professionals and patients seeking detailed information regarding its pharmacological profile, therapeutic application, and safety considerations.
1. Mechanism of Action
Aclasta functions primarily as an inhibitor of bone resorption. Its mechanism is highly sophisticated, targeting the cellular pathways of osteoclasts—the cells responsible for the breakdown of bone tissue.
Cellular Pathways
- Osteoclast Inhibition: Zoledronic acid localizes to areas of high bone turnover. Once internalized by osteoclasts, it inhibits the enzyme farnesyl pyrophosphate synthase (FPPS).
- Protein Prenylation: By inhibiting FPPS, Aclasta prevents the prenylation of small GTPase signaling proteins (such as Ras, Rho, and Rac). These proteins are essential for osteoclast cytoskeleton organization, membrane ruffling, and cell survival.
- Apoptosis Induction: The loss of these signaling proteins leads to a loss of osteoclast function and eventually triggers apoptosis (programmed cell death).
This process effectively slows the rate of bone remodeling, resulting in a net increase in bone mineral density (BMD) and a reduction in the risk of fracture.
2. Pharmacokinetics
Understanding the pharmacokinetic profile of Aclasta is essential for managing its administration and potential systemic effects.
| Parameter | Description |
|---|---|
| Administration | Intravenous infusion (typically over 15 minutes). |
| Distribution | Rapidly binds to bone mineral; approximately 56% bound to plasma proteins. |
| Metabolism | Not metabolized in the human body. |
| Excretion | Excreted unchanged by the kidneys (renal clearance). |
| Half-life | Terminal elimination half-life is prolonged due to bone binding, lasting several days to weeks. |
3. Clinical Indications and Usage
Aclasta is indicated for several distinct skeletal pathologies. Its once-yearly or once-every-two-years dosing schedule (depending on the condition) offers significant advantages in patient compliance.
Primary Indications
- Postmenopausal Osteoporosis: Treatment to reduce the incidence of hip, vertebral, and non-vertebral fractures.
- Osteoporosis in Men: To increase bone mass in men with primary osteoporosis.
- Glucocorticoid-Induced Osteoporosis: Prevention and treatment in patients initiating or continuing long-term systemic glucocorticoid therapy.
- Paget’s Disease of Bone: Treatment of patients with elevated alkaline phosphatase levels or those at risk of complications.
- Prevention of Clinical Fractures after Hip Fracture: Reducing the risk of subsequent fractures in patients who have suffered a low-trauma hip fracture.
4. Dosage and Administration Guidelines
Aclasta must be administered by a healthcare professional via intravenous infusion.
- Standard Dose: 5 mg infusion administered over no less than 15 minutes.
- Preparation: The solution should be at room temperature before administration. It must not be mixed with calcium-containing or other divalent cation-containing solutions (e.g., Lactated Ringer’s).
- Hydration: Patients must be adequately hydrated before and after the administration of Aclasta to minimize the risk of renal complications.
5. Contraindications and Risks
Absolute Contraindications
- Hypersensitivity: Known clinical hypersensitivity to zoledronic acid or any bisphosphonate.
- Hypocalcemia: Must be corrected before starting Aclasta therapy.
- Renal Impairment: Patients with severe renal impairment (Creatinine Clearance < 35 mL/min).
- Pregnancy/Lactation: Aclasta is contraindicated due to potential fetal harm.
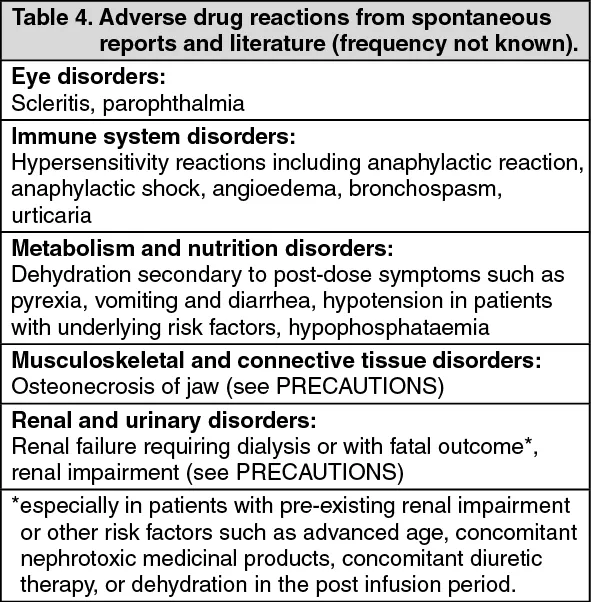
Key Risks and Side Effects
- Acute Phase Reaction: Many patients experience flu-like symptoms (fever, myalgia, arthralgia) within the first 3 days post-infusion.
- Osteonecrosis of the Jaw (ONJ): Rare but serious. Patients should undergo a dental examination prior to treatment.
- Atypical Femoral Fractures: Long-term bisphosphonate use has been associated with subtrochanteric and diaphyseal femoral fractures.
- Renal Toxicity: Risk of renal function decline, especially in patients with pre-existing renal disease or concurrent use of nephrotoxic drugs.
6. Drug Interactions
Clinical caution is advised when Aclasta is co-administered with:
1. Aminoglycosides: Potential for prolonged hypocalcemia.
2. Nephrotoxic Agents: Increased risk of renal impairment.
3. Loop Diuretics: May increase the risk of hypocalcemia.
7. Pregnancy and Lactation Warnings
Aclasta is categorized as a drug that poses significant risks to a developing fetus. Bisphosphonates are incorporated into the bone matrix and released gradually over years. Therefore, women of childbearing potential should use effective contraception during treatment and for a period after discontinuation. Aclasta should not be used during breastfeeding as there is no data on its excretion into human milk.
8. Overdose Management
Acute overdose of Aclasta is rare due to the controlled clinical setting of administration. However, in cases of inadvertent overdose:
* Clinical Monitoring: Monitor serum calcium, phosphate, and magnesium levels.
* Hypocalcemia: If significant hypocalcemia occurs, administer intravenous calcium gluconate or calcium chloride.
* Renal Function: Monitor renal function closely, as high doses may lead to renal failure.
9. Frequently Asked Questions (FAQ)
1. How often do I need to receive an Aclasta infusion?
For osteoporosis, it is typically administered once every 12 months. For Paget’s disease, a single dose is often sufficient, though retreatment may be necessary based on biochemical markers.
2. Can I take calcium supplements with Aclasta?
Yes, it is standard practice to ensure adequate daily intake of calcium and Vitamin D to prevent hypocalcemia, unless contraindicated by your physician.
3. What should I do if I miss a dose?
Contact your healthcare provider immediately to reschedule. The timing of the infusion is important for maintaining bone density.
4. Is Aclasta painful to receive?
The infusion itself is not painful. However, many patients report flu-like symptoms (fever, body aches) 24–72 hours after the infusion.
5. How long does it take for Aclasta to work?
Aclasta begins to reduce bone turnover markers within days, but the clinical reduction in fracture risk is cumulative over the course of the treatment year.
6. Are there specific dental precautions?
Yes. It is highly recommended to complete any necessary dental procedures (extractions, implants) before starting Aclasta to reduce the risk of ONJ.
7. Does Aclasta affect my kidneys?
Aclasta is cleared by the kidneys. If you have pre-existing kidney disease, your doctor will likely monitor your creatinine levels closely before and after the infusion.
8. Can I drive after receiving an Aclasta infusion?
Yes, there are no specific restrictions on driving, though you may feel tired or have muscle aches post-infusion.
9. How is Aclasta different from oral bisphosphonates?
Aclasta is administered intravenously once a year, eliminating the need for daily or weekly oral dosing and avoiding common gastrointestinal side effects associated with oral bisphosphonates.
10. Can I stop taking Aclasta after one year?
Treatment duration is determined by your physician based on your fracture risk, bone density scans (DEXA), and response to therapy. Do not discontinue treatment without medical consultation.
Conclusion
Aclasta remains a cornerstone in the pharmacological management of osteoporosis and other skeletal disorders. Its efficacy in reducing fracture risk, combined with the convenience of annual dosing, makes it a preferred option for many patients. However, patient safety—specifically regarding renal health and dental hygiene—must remain a priority throughout the duration of the therapy. Always consult with your orthopedic specialist or endocrinologist to determine if Aclasta is the right treatment plan for your specific clinical profile.
Disclaimer: This guide is for educational purposes only and does not constitute medical advice. Always consult with a qualified healthcare professional regarding medical conditions or treatment plans.