

Comprehensive Guide to Pantoscot: Clinical Pharmacology and Therapeutic Applications
In the landscape of gastrointestinal pharmacology, Proton Pump Inhibitors (PPIs) remain the gold standard for managing acid-related disorders. Pantoscot, a widely prescribed medication containing Pantoprazole, stands at the forefront of this therapeutic class. This guide serves as an authoritative reference for healthcare professionals and patients seeking a deep understanding of its pharmacological profile, clinical utility, and safety considerations.
1. Introduction and Overview
Pantoscot is a substituted benzimidazole derivative that functions as a potent inhibitor of gastric acid secretion. By targeting the H+/K+-ATPase enzyme system—the final step in the gastric acid production pathway—Pantoscot provides rapid and sustained relief from conditions exacerbated by hyperacidity.
Unlike H2-receptor antagonists, which only partially block acid production, Pantoscot effectively shuts down the "proton pump" in the parietal cells of the stomach lining. This makes it a cornerstone therapy for conditions ranging from simple gastroesophageal reflux disease (GERD) to complex cases of Zollinger-Ellison syndrome.
2. Technical Specifications and Mechanism of Action
The Proton Pump Mechanism
The efficacy of Pantoscot is rooted in its unique pharmacodynamic profile. The drug is a prodrug that requires activation in an acidic environment.
- Absorption: Upon oral administration, Pantoscot is absorbed in the small intestine.
- Activation: The drug travels through the bloodstream to the secretory canaliculi of the gastric parietal cells. Here, in the highly acidic environment (pH < 3.0), the drug undergoes a structural transformation into its active form, a cyclic sulfenamide.
- Binding: The active metabolite binds covalently to the H+/K+-ATPase enzyme (the proton pump). This bond is irreversible, meaning the enzyme is permanently disabled for the remainder of its lifespan.
- Inhibition: Acid secretion resumes only after the parietal cell synthesizes new proton pumps, which typically takes 24 to 48 hours.
Pharmacokinetics
| Parameter | Description |
|---|---|
| Bioavailability | Approximately 77% |
| Protein Binding | Highly bound to albumin (~98%) |
| Metabolism | Extensive hepatic metabolism via CYP2C19 |
| Half-life | Approximately 1 to 2 hours |
| Excretion | Primarily renal (80%), with the remainder via feces |
3. Clinical Indications and Usage
Pantoscot is indicated for a variety of gastrointestinal pathologies where the reduction of gastric acid is clinically necessary.
Primary Indications
- Gastroesophageal Reflux Disease (GERD): Treatment of erosive esophagitis and associated symptoms such as heartburn and acid regurgitation.
- Peptic Ulcer Disease (PUD): Healing of gastric and duodenal ulcers.
- Helicobacter pylori Eradication: Used in combination with specific antibiotics (e.g., clarithromycin, amoxicillin) to treat H. pylori infections.
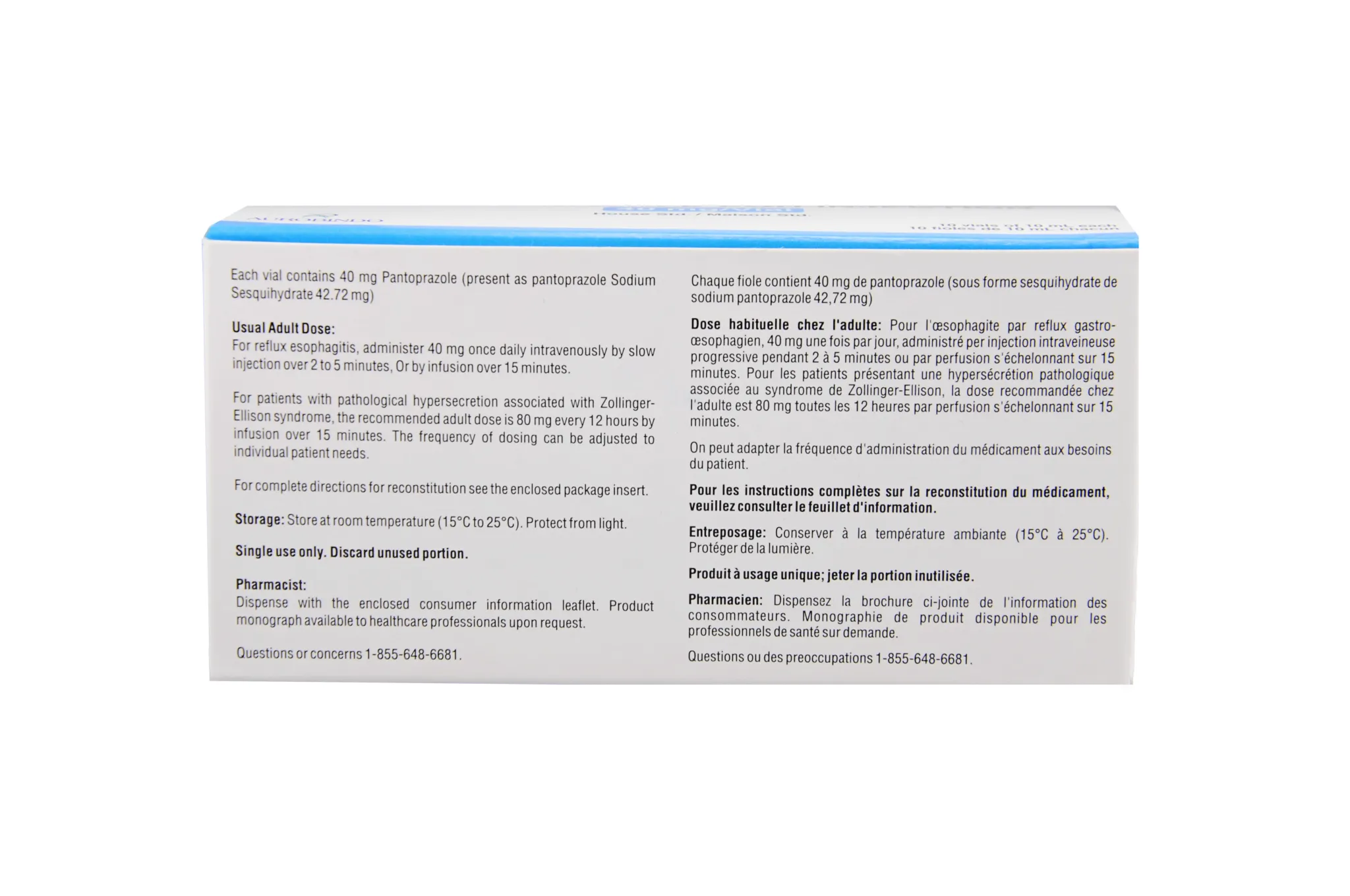
- Zollinger-Ellison Syndrome: Pathological hypersecretory conditions.
- NSAID-Induced Ulcer Prophylaxis: Used in patients requiring chronic NSAID therapy to prevent mucosal injury.
Dosage Guidelines
Note: Dosage must be individualized based on the patient's condition and renal/hepatic function.
| Condition | Recommended Dosage |
|---|---|
| Erosive Esophagitis | 40 mg once daily for 8 weeks |
| Duodenal Ulcer | 40 mg daily for 2–4 weeks |
| GERD Maintenance | 20–40 mg daily |
| Zollinger-Ellison | 40 mg twice daily (up to 240 mg/day if needed) |
4. Risks, Side Effects, and Contraindications
While generally well-tolerated, Pantoscot carries specific risks that necessitate clinical monitoring.
Common Side Effects
- Headache
- Diarrhea or constipation
- Nausea and abdominal pain
- Dizziness
Serious Adverse Events (Rare)
- Hypomagnesemia: Long-term PPI use can lead to magnesium deficiency, manifesting as muscle tremors or arrhythmias.
- Bone Fractures: Potential association with increased risk of osteoporosis-related fractures in high-dose, long-term users.
- Vitamin B12 Deficiency: Chronic acid suppression can impair the absorption of B12.
- Clostridioides difficile Infection: Altered gut pH may increase susceptibility to enteric infections.
Contraindications
- Hypersensitivity: Known allergy to Pantoprazole or any component of the formulation.
- Co-administration with Rilpivirine: PPIs significantly decrease the plasma concentration of this antiretroviral drug.
5. Pregnancy, Lactation, and Special Populations
- Pregnancy: Pantoscot is classified as FDA Pregnancy Category B. It should only be used if clearly needed and under the direction of a physician.
- Lactation: Data on excretion into breast milk is limited; caution is advised.
- Hepatic Impairment: Dose adjustment may be required in patients with severe liver disease.
6. Drug Interactions
Pantoscot interacts with medications that rely on gastric pH for absorption or those metabolized by the CYP450 enzyme system.
- Ketoconazole/Itraconazole: Reduced absorption due to increased gastric pH.
- Warfarin: Monitor INR closely, as PPIs may increase the anticoagulant effect.
- Methotrexate: Potential for increased serum levels, leading to toxicity.
- Clopidogrel: Potential reduction in the antiplatelet effect of clopidogrel (though clinical significance is debated).
7. Overdose Management
There is no specific antidote for Pantoscot overdose. In cases of intentional or accidental ingestion exceeding recommended doses, management is primarily supportive:
1. Gastric Lavage: If ingestion is recent.
2. Symptomatic Support: Monitor vitals and provide intravenous fluids.
3. Hemodialysis: Pantoscot is not significantly removed by hemodialysis due to high protein binding.
8. Frequently Asked Questions (FAQ)
1. Is Pantoscot the same as Omeprazole?
Both are Proton Pump Inhibitors, but they have different chemical structures and metabolic pathways. Pantoscot (Pantoprazole) is often preferred for its lower potential for drug-drug interactions compared to Omeprazole.
2. Should I take Pantoscot before or after food?
For optimal absorption, Pantoscot should be taken approximately 30 to 60 minutes before a meal, typically breakfast.
3. Can I crush or chew the tablets?
No. Pantoscot tablets are enteric-coated to protect the active ingredient from stomach acid. Crushing or chewing destroys this coating, rendering the medication ineffective.
4. How long can I safely take Pantoscot?
Long-term use should only be under medical supervision. If used for more than one year, your doctor should monitor your magnesium, calcium, and B12 levels.
5. What should I do if I miss a dose?
Take the missed dose as soon as you remember. If it is almost time for your next dose, skip the missed one. Do not take a double dose to catch up.
6. Does Pantoscot cause weight gain?
Weight gain is not a recognized side effect of Pantoscot. If you experience unexplained weight changes, consult your healthcare provider.
7. Can I drink alcohol while taking this medication?
Alcohol can increase gastric acid production and irritate the stomach lining, potentially negating the benefits of the medication. It is best to avoid alcohol during treatment.
8. Is Pantoscot addictive?
No, Pantoscot does not cause physical or psychological dependence. However, stopping it suddenly after long-term use may cause "rebound acid hypersecretion."
9. Why am I still experiencing heartburn while on Pantoscot?
If symptoms persist, it may indicate a dosage issue, an incorrect diagnosis, or the presence of H. pylori. Consult your doctor for a reassessment.
10. Can children take Pantoscot?
Pediatric use is generally restricted to specific conditions and age groups. It should only be administered under strict pediatric supervision.
Disclaimer: This guide is for educational purposes only and does not constitute medical advice. Always consult with a licensed physician or pharmacist before starting, stopping, or altering any medication regimen.