
Comprehensive Guide to Multivitamins with Minerals: Clinical Perspectives
In the modern landscape of nutritional science and orthopedic medicine, the role of micronutrient supplementation has transitioned from a general wellness recommendation to a targeted therapeutic intervention. A "Multivitamin with Minerals" represents a complex formulation designed to bridge the gap between dietary intake and the physiological requirements necessary for optimal homeostatic function, bone density maintenance, and cellular repair.
This guide provides an exhaustive clinical overview of these formulations, serving as a resource for healthcare practitioners and patients seeking to understand the pharmacological and physiological impact of supplemental micronutrients.
1. Mechanism of Action: The Biochemical Foundation
Multivitamins with minerals function by providing essential cofactors, coenzymes, and structural elements that the human body cannot synthesize in sufficient quantities.
Metabolic Catalysis
Most vitamins (specifically the B-complex group) act as coenzymes in enzymatic reactions. For instance, Thiamine (B1), Riboflavin (B2), and Niacin (B3) are critical for the Krebs cycle and oxidative phosphorylation, facilitating the conversion of macronutrients (carbohydrates, fats, and proteins) into Adenosine Triphosphate (ATP).
Mineral Homeostasis and Structural Integrity
Minerals provided in these supplements, such as Calcium, Magnesium, and Zinc, serve dual roles:
* Structural: Calcium and Phosphorus are the primary constituents of the hydroxyapatite matrix in bone tissue.
* Regulatory: Magnesium acts as a cofactor for over 300 enzymatic reactions, including those involved in muscle contraction and nerve impulse transmission—critical for orthopedic rehabilitation.
* Antioxidant Defense: Selenium, Vitamin C, and Vitamin E function to neutralize reactive oxygen species (ROS), thereby mitigating systemic inflammation and oxidative stress at the cellular level.
2. Pharmacokinetics: Absorption and Distribution
The pharmacokinetics of a multivitamin with minerals are complex due to the varying solubilities and chemical forms of the individual components.
| Component Type | Absorption Mechanism | Primary Storage Site |
|---|---|---|
| Water-Soluble (B, C) | Facilitated diffusion/Active transport | Minimal (Excreted in urine) |
| Fat-Soluble (A, D, E, K) | Micellar solubilization/Lymphatic uptake | Liver and Adipose tissue |
| Minerals (Fe, Zn, Ca) | Ion channels/Carrier proteins | Bone matrix, Liver, Blood |
- Bioavailability: Absorption is heavily dependent on the presence of dietary fat (for fat-soluble vitamins) and gastric pH levels.
- Metabolism: Many vitamins undergo hepatic conversion into their active coenzyme forms (e.g., Pyridoxine to Pyridoxal 5'-phosphate).
- Excretion: Water-soluble components are primarily excreted via the renal system, necessitating regular intake. Fat-soluble vitamins have a longer half-life and carry a higher risk of toxicity if consumed in excess.
3. Clinical Indications and Therapeutic Usage
Multivitamins with minerals are indicated for patients with inadequate dietary intake, metabolic absorption disorders, or increased physiological demands.
Orthopedic and Musculoskeletal Indications
In the field of orthopedics, specific micronutrients are essential for recovery:
1. Post-Fracture Healing: Calcium, Vitamin D3, and Magnesium are indicated to promote osteoblast activity and bone mineralization.
2. Chronic Inflammation: Zinc and Vitamin C are utilized to support collagen synthesis and connective tissue repair following surgical procedures.
3. Muscle Function: Adequate levels of Magnesium and Potassium are necessary to prevent muscle spasms and support neuromuscular health post-immobilization.
General Indications
- Geriatric Populations: To address age-related malabsorption and decreased caloric intake.
- Post-Bariatric Surgery: Due to significant reduction in nutrient absorption surface area.
- Pregnancy and Lactation: To support fetal development and increased maternal metabolic rate.
4. Risks, Side Effects, and Contraindications
While generally safe, the "more is better" philosophy can lead to adverse clinical outcomes.
Potential Side Effects
- Gastrointestinal: Nausea, constipation (often attributed to Iron or Calcium supplements), and abdominal cramping.
- Dermatological: Flushing (Niacin) or skin rashes.
- Renal: Hypercalciuria, which may increase the risk of nephrolithiasis (kidney stones).
Contraindications
- Hypervitaminosis: Individuals with pre-existing high levels of fat-soluble vitamins (A, D, E, K).
- Hemochromatosis: Patients with iron overload disorders must avoid formulations containing Iron.
- Renal Failure: Patients with compromised renal function require specialized formulations, as they cannot effectively excrete excess minerals.
5. Drug Interactions: Critical Safety Warnings
Healthcare providers must screen for potential interactions, as minerals can significantly alter the pharmacokinetics of prescription medications.
- Antibiotics: Calcium, Magnesium, and Iron can chelate with Tetracyclines and Fluoroquinolones, rendering them ineffective. A 2–4 hour gap is required.
- Anticoagulants: Vitamin K antagonizes the effects of Warfarin. Patients on blood thinners must maintain consistent Vitamin K intake.
- Levothyroxine: Calcium and Iron supplements interfere with the absorption of thyroid hormones.
6. Pregnancy and Lactation
Micronutrient requirements increase significantly during gestation. However, supplementation must be supervised:
* Vitamin A: High doses of preformed Vitamin A (retinol) are teratogenic. Prenatal formulations typically use Beta-carotene.
* Folic Acid: Essential for preventing neural tube defects; supplementation should ideally begin pre-conception.
* Iron: Necessary for increased maternal blood volume but should be balanced to avoid gastrointestinal distress.
7. Overdose Management
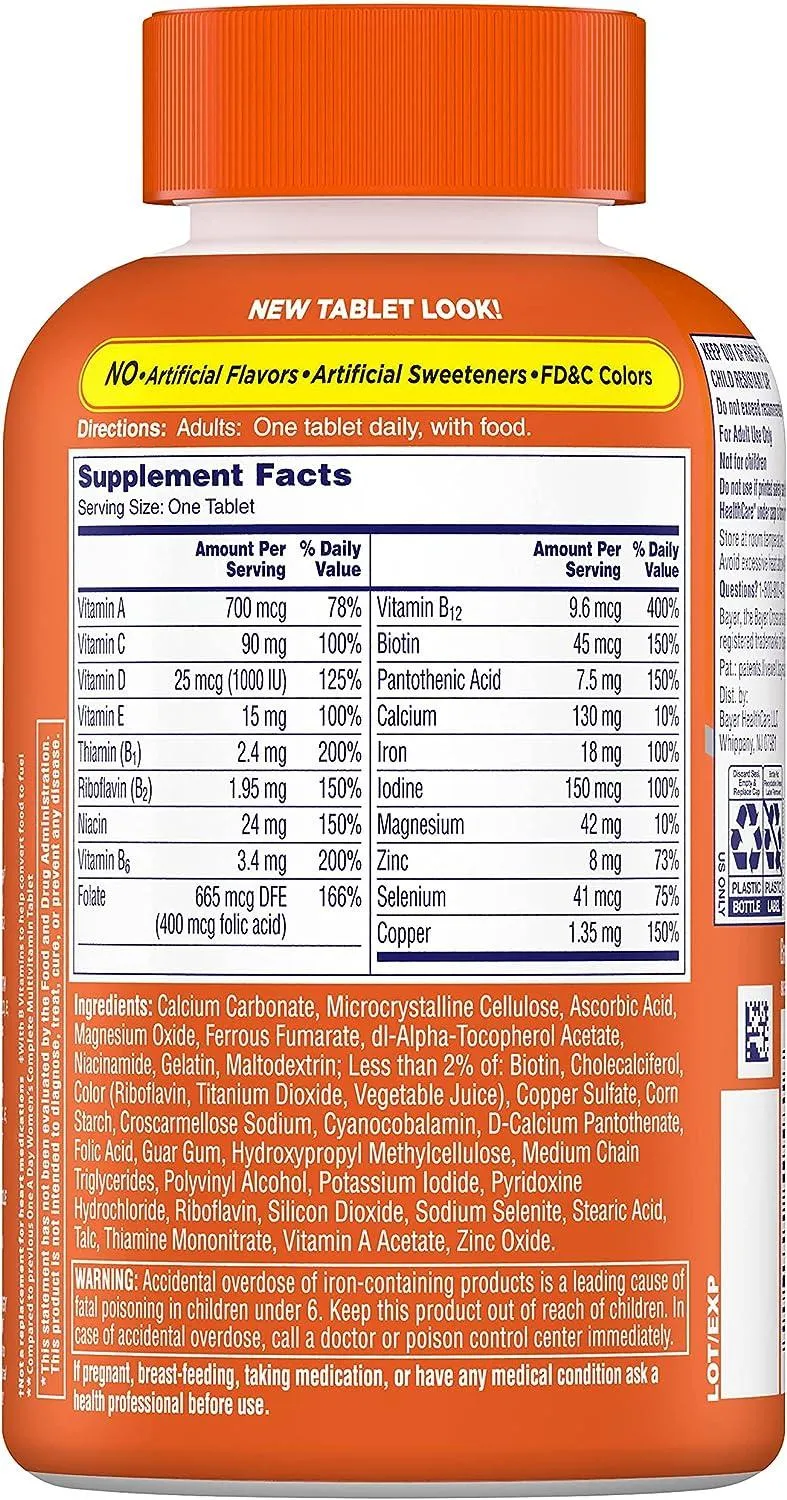
Acute toxicity is rare but possible, particularly with Iron-containing multivitamins, which are a leading cause of pediatric poisoning.
- Iron Toxicity: Presents with severe abdominal pain, vomiting, diarrhea, and potential cardiovascular collapse. Treatment includes gastric lavage and chelation therapy (e.g., Deferoxamine).
- Fat-Soluble Toxicity: Chronic high-dose Vitamin A or D intake can lead to systemic toxicity, including hepatic damage or hypercalcemia.
- Emergency Protocol: In cases of suspected overdose, immediate contact with a Poison Control Center or emergency department is mandatory.
8. Frequently Asked Questions (FAQ)
1. Can I take a multivitamin on an empty stomach?
While many people do, it is generally recommended to take multivitamins with a meal to improve the absorption of fat-soluble vitamins and reduce gastrointestinal irritation.
2. Do multivitamins replace a healthy diet?
No. They are intended as a supplement to, not a replacement for, a balanced diet. Whole foods provide fiber, phytonutrients, and a synergy of compounds that supplements cannot replicate.
3. Why does my urine turn bright yellow after taking a multivitamin?
This is usually due to Riboflavin (Vitamin B2), which is naturally yellow-fluorescent and is excreted in the urine. It is harmless.
4. Is there a "best" time of day to take them?
Morning is often preferred to ensure consistency and to provide the body with metabolic cofactors at the start of the daily activity cycle.
5. Can multivitamins cause kidney stones?
Excessive intake of Calcium and Vitamin C (which metabolizes into oxalate) may increase the risk of calcium-oxalate stones in susceptible individuals.
6. Are synthetic vitamins as good as natural ones?
Most vitamins in supplements are chemically identical to those found in food. However, natural food sources provide superior bioavailability and co-nutrients.
7. How long does it take for a multivitamin to "work"?
Multivitamins are not immediate-acting drugs. Depending on the deficiency, it may take weeks or months of consistent use to see improvements in blood markers or energy levels.
8. Can I take a multivitamin while on prescription medication?
Always consult your physician. As noted, minerals like iron and calcium can interfere with the absorption of many common medications.
9. What is the difference between a "multivitamin" and a "prenatal"?
Prenatal vitamins are specifically formulated with higher levels of Folic Acid, Iron, and Iodine to meet the needs of a developing fetus, often with lower levels of Vitamin A.
10. Should athletes take extra minerals?
Athletes may have higher requirements for magnesium, zinc, and electrolytes due to sweat loss. However, they should avoid excessive supplementation without blood work, as mineral imbalances can impair performance.
Conclusion
Multivitamins with minerals are powerful tools for maintaining physiological homeostasis, particularly in the context of orthopedic recovery and general health optimization. By understanding the mechanisms of action, respecting the pharmacokinetic limitations, and adhering to strict clinical guidelines, patients and providers can utilize these formulations to achieve significant health outcomes. Always prioritize professional medical advice tailored to individual blood markers and clinical history before initiating long-term supplementation.