

Comprehensive Guide to High-Dose Vitamin D3 (50,000 IU)
Vitamin D3, or cholecalciferol, is a secosteroid hormone essential for human health, particularly in orthopedic and metabolic stability. While standard daily supplements typically range from 600 to 2,000 IU, the high-dose 50,000 IU formulation is a clinical therapeutic intervention used exclusively for the treatment of severe vitamin D deficiency. This guide provides an exhaustive clinical overview of its pharmacological profile, indications, and safety parameters.
1. Mechanism of Action and Pharmacokinetics
The Biological Pathway
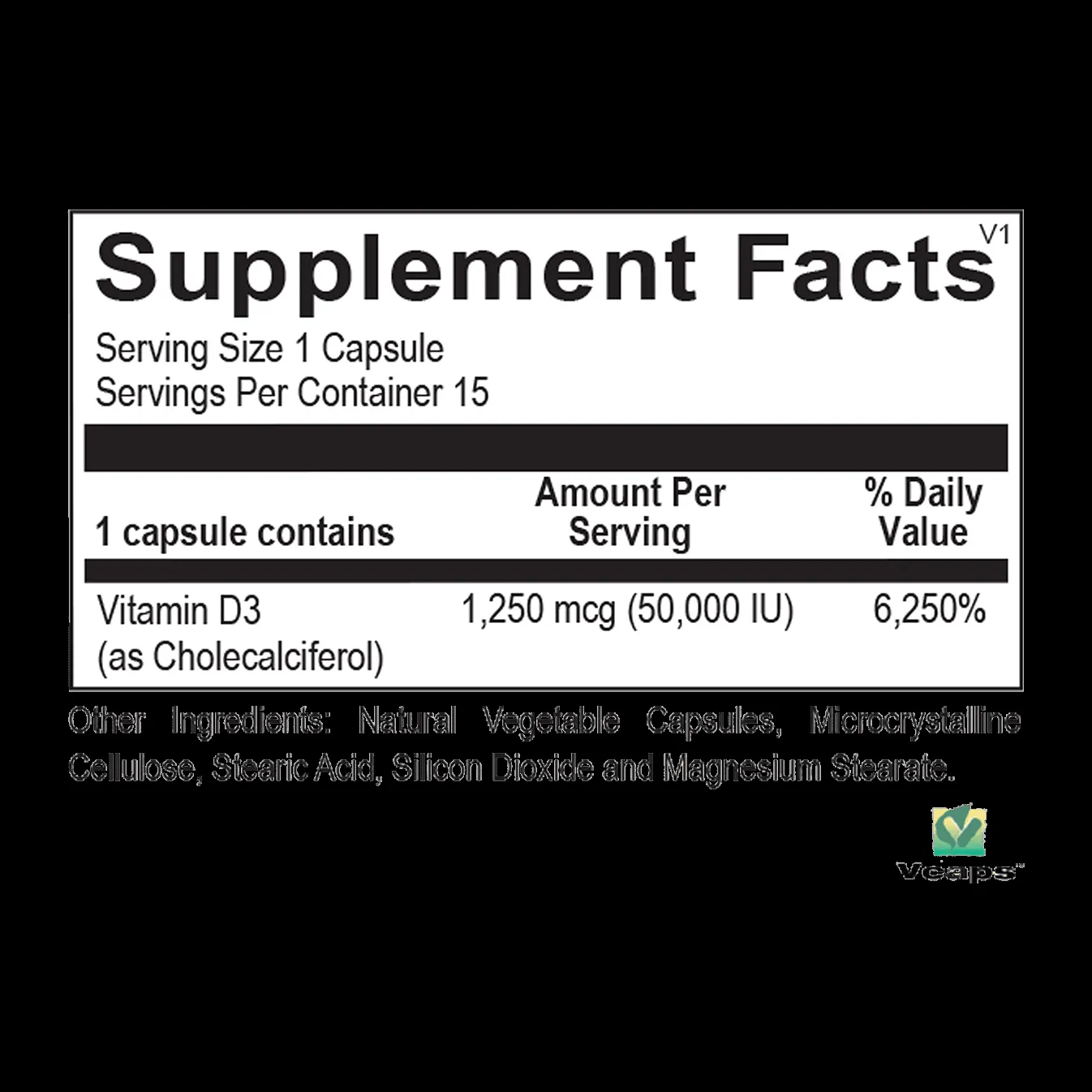
Vitamin D3 is not merely a vitamin; it functions as a prohormone. When administered orally, cholecalciferol undergoes a two-step hydroxylation process:
1. Hepatic Hydroxylation: In the liver, cholecalciferol is converted to 25-hydroxyvitamin D [25(OH)D], also known as calcidiol. This is the primary circulating form of the vitamin and is the standard marker used to assess a patient's vitamin D status.
2. Renal Hydroxylation: In the kidneys, 25(OH)D is converted by the enzyme 1-alpha-hydroxylase into 1,25-dihydroxyvitamin D [1,25(OH)2D], or calcitriol. This is the biologically active form of the hormone.
Physiological Function
The active form of Vitamin D3 binds to the Vitamin D Receptor (VDR), a nuclear transcription factor found in almost every cell in the human body. Its primary roles include:
* Calcium Homeostasis: Enhancing the intestinal absorption of calcium and phosphorus.
* Bone Remodeling: Facilitating osteoblast activity and maintaining the mineralization of the osteoid matrix.
* Immunomodulation: Regulating T-cell function and cytokine production.
Pharmacokinetics
- Absorption: Vitamin D3 is fat-soluble and requires dietary fat for optimal absorption in the small intestine.
- Distribution: It is transported in the blood bound to Vitamin D-binding protein (DBP).
- Half-life: The circulating 25(OH)D has a half-life of approximately 15 days to 3 weeks, which allows for the intermittent dosing schedule characteristic of the 50,000 IU regimen.
2. Clinical Indications and Therapeutic Usage
The 50,000 IU dosage is reserved for patients who have been diagnosed with clinically significant Vitamin D deficiency (typically serum levels < 20 ng/mL).
Primary Indications
| Indication | Clinical Context |
|---|---|
| Severe Deficiency | Serum levels below 20 ng/mL, often associated with bone pain or muscle weakness. |
| Osteomalacia | Softening of the bones due to defective bone mineralization. |
| Hypocalcemia | Used in conjunction with calcium supplementation to restore mineral balance. |
| Malabsorption Syndromes | Used in patients with Crohn’s disease, Celiac disease, or post-gastric bypass who cannot absorb standard doses. |
Standard Dosing Protocols
Clinical practice guidelines (such as those from the Endocrine Society) suggest that for adult patients with deficiency, a common therapeutic regimen includes:
* Loading Phase: 50,000 IU once weekly for 8 to 12 weeks.
* Maintenance Phase: After the 8-12 week period, serum levels should be re-tested. If levels are normalized (typically >30 ng/mL), the patient is transitioned to a daily maintenance dose of 1,500–2,000 IU.
3. Contraindications, Interactions, and Warnings
High-dose Vitamin D3 is a potent intervention. Before prescribing, practitioners must evaluate the patient’s existing metabolic profile.
Absolute Contraindications
- Hypercalcemia: Elevated calcium levels in the blood.
- Hypervitaminosis D: Existing toxicity.
- Nephrolithiasis: A history of calcium-based kidney stones.
- Hypersensitivity: Known allergic reactions to cholecalciferol or the vehicle oil (often soybean or peanut oil).
Significant Drug Interactions
| Interacting Agent | Potential Effect |
|---|---|
| Digoxin | Increased risk of cardiac arrhythmias due to hypercalcemia. |
| Thiazide Diuretics | Risk of hypercalcemia due to increased renal calcium reabsorption. |
| Orlistat | Inhibits the absorption of fat-soluble vitamins, reducing D3 efficacy. |
| Corticosteroids | Can increase the metabolism of Vitamin D, potentially leading to lower serum levels. |
Pregnancy and Lactation
Vitamin D3 is categorized as generally safe during pregnancy, but the 50,000 IU dose should only be used if the benefit outweighs the risk. Excessive doses during pregnancy can theoretically lead to fetal hypercalcemia. Breastfeeding mothers require Vitamin D supplementation, but high-dose regimens should be monitored by an obstetrician.
4. Overdose Management and Toxicity
Vitamin D toxicity, or hypervitaminosis D, is characterized by excessive calcium levels (hypercalcemia) in the blood.
Symptoms of Toxicity
- Early signs: Nausea, vomiting, constipation, polyuria (excessive urination), and polydipsia (excessive thirst).
- Advanced signs: Kidney stones, nephrocalcinosis, cardiac arrhythmias, and confusion.
Management Protocols
If overdose is suspected:
1. Discontinuation: Immediately stop the administration of the 50,000 IU supplement.
2. Serum Testing: Measure serum 25(OH)D and serum calcium levels immediately.
3. Hydration: Aggressive fluid therapy to promote calcium excretion.
4. Dietary Modification: Restrict calcium intake until levels return to the reference range.
5. Medical Intervention: In severe cases, corticosteroids or calcitonin may be utilized to lower serum calcium.
5. Frequently Asked Questions (FAQ)
1. Why is 50,000 IU only taken weekly rather than daily?
Because Vitamin D3 is fat-soluble and has a long half-life, a high dose once a week provides a sustained release and steady serum concentration without the risk of daily overdose.
2. Should I take this with food?
Yes. Since Vitamin D3 is fat-soluble, taking it with a meal that contains healthy fats (e.g., avocado, nuts, or dairy) significantly improves absorption.
3. Will this cure my bone pain?
If the bone pain is caused specifically by vitamin D deficiency-induced osteomalacia, then yes, replenishing your levels will resolve the symptoms. However, it will not cure other orthopedic conditions like osteoarthritis.
4. How long does it take for my levels to rise?
Most patients see a significant increase in serum 25(OH)D levels after 4 to 8 weeks of consistent weekly dosing.
5. Can I take this if I have high blood pressure?
Generally, yes. However, if you are taking thiazide diuretics for your blood pressure, you must inform your doctor, as the combination can lead to hypercalcemia.
6. Are there specific side effects I should watch for?
Most people tolerate it well. However, watch for symptoms of high calcium: constipation, persistent nausea, or unexplained fatigue.
7. Do I need to take extra calcium with this?
Your doctor may recommend a calcium supplement if your dietary intake is low. Do not start high-dose calcium without medical supervision, as it increases the risk of kidney stones.
8. What happens if I miss a dose?
If you miss a weekly dose, take it as soon as you remember. If it is almost time for your next dose, skip the missed one. Do not take two doses at once.
9. Is this supplement "natural"?
Vitamin D3 (cholecalciferol) is the same form of vitamin D produced by the human skin when exposed to sunlight.
10. Can I stay on the 50,000 IU dose forever?
No. This is a therapeutic loading dose. Long-term use of 50,000 IU weekly without active deficiency can lead to toxicity. You must transition to a maintenance dose once your levels are corrected.
Conclusion
Vitamin D3 50,000 IU is a vital tool in the medical management of severe deficiency. When used under the guidance of a healthcare professional, it effectively restores calcium homeostasis and improves bone mineral density. Patients should prioritize regular blood monitoring to ensure safe levels and prevent the complications associated with hypervitaminosis D. Always consult with your orthopedic specialist or primary care provider before beginning this high-intensity regimen.
Disclaimer: This content is for educational purposes only and does not constitute medical advice. Always consult with a licensed healthcare professional before starting any new medication or dosage regimen.