



Comprehensive Guide to Vitamin D3 (Cholecalciferol)
Vitamin D3, or cholecalciferol, is a secosteroid hormone precursor that plays a fundamental role in human physiology. While colloquially referred to as a "vitamin," its systemic impact—particularly on musculoskeletal integrity and immunomodulation—classifies it as a vital hormone. In orthopedic medicine, Vitamin D3 is the cornerstone of bone metabolism, essential for the intestinal absorption of calcium and the maintenance of serum phosphate levels.
This guide provides an exhaustive clinical overview of Vitamin D3, designed for healthcare professionals and patients seeking a rigorous, evidence-based understanding of its pharmacokinetics, indications, and safety profile.
Mechanism of Action and Pharmacokinetics
Biological Pathway
Vitamin D3 is synthesized in the skin via the photochemical conversion of 7-dehydrocholesterol upon exposure to ultraviolet B (UVB) radiation. Once synthesized or ingested, it undergoes a two-step activation process:
- Hepatic Hydroxylation: In the liver, Vitamin D3 is converted by the enzyme 25-hydroxylase into 25-hydroxyvitamin D [25(OH)D], also known as calcifediol. This is the primary circulating form used to assess vitamin D status.
- Renal Hydroxylation: In the kidneys, 25(OH)D is further converted by 1-alpha-hydroxylase into 1,25-dihydroxyvitamin D [1,25(OH)2D], or calcitriol—the biologically active hormone.
Molecular Mechanism
Calcitriol binds to the Vitamin D Receptor (VDR), a nuclear transcription factor. This complex regulates the expression of genes involved in:
* Calcium Homeostasis: Enhancing the expression of calcium-binding proteins (calbindins) in the intestinal epithelium.
* Bone Remodeling: Regulating osteoblast and osteoclast activity to ensure proper mineralization of the osteoid matrix.
* Cellular Signaling: Modulating immune response through the regulation of cytokines and antimicrobial peptides.
Pharmacokinetics
- Absorption: Passive diffusion in the small intestine, facilitated by dietary fats.
- Distribution: Transported in the blood via Vitamin D-Binding Protein (DBP).
- Metabolism: Primarily hepatic and renal.
- Excretion: Primarily via bile and feces; minimal renal excretion.
- Half-life: The half-life of 25(OH)D is approximately 15 to 30 days, allowing for intermittent dosing regimens.
Clinical Indications and Usage
Vitamin D3 is indicated for the prevention and treatment of various conditions characterized by deficiency or impaired metabolism.
| Indication | Clinical Significance |
|---|---|
| Osteomalacia | Treatment of bone softening due to severe deficiency. |
| Osteoporosis | Adjunct therapy to calcium to improve bone mineral density. |
| Hypoparathyroidism | Management of calcium balance in deficient states. |
| Rickets | Treatment and prevention of childhood bone deformities. |
| Chronic Kidney Disease | Managing secondary hyperparathyroidism (under specialist supervision). |
Dosage Guidelines
Dosage must be individualized based on serum 25(OH)D levels. General clinical practice follows the Endocrine Society guidelines:
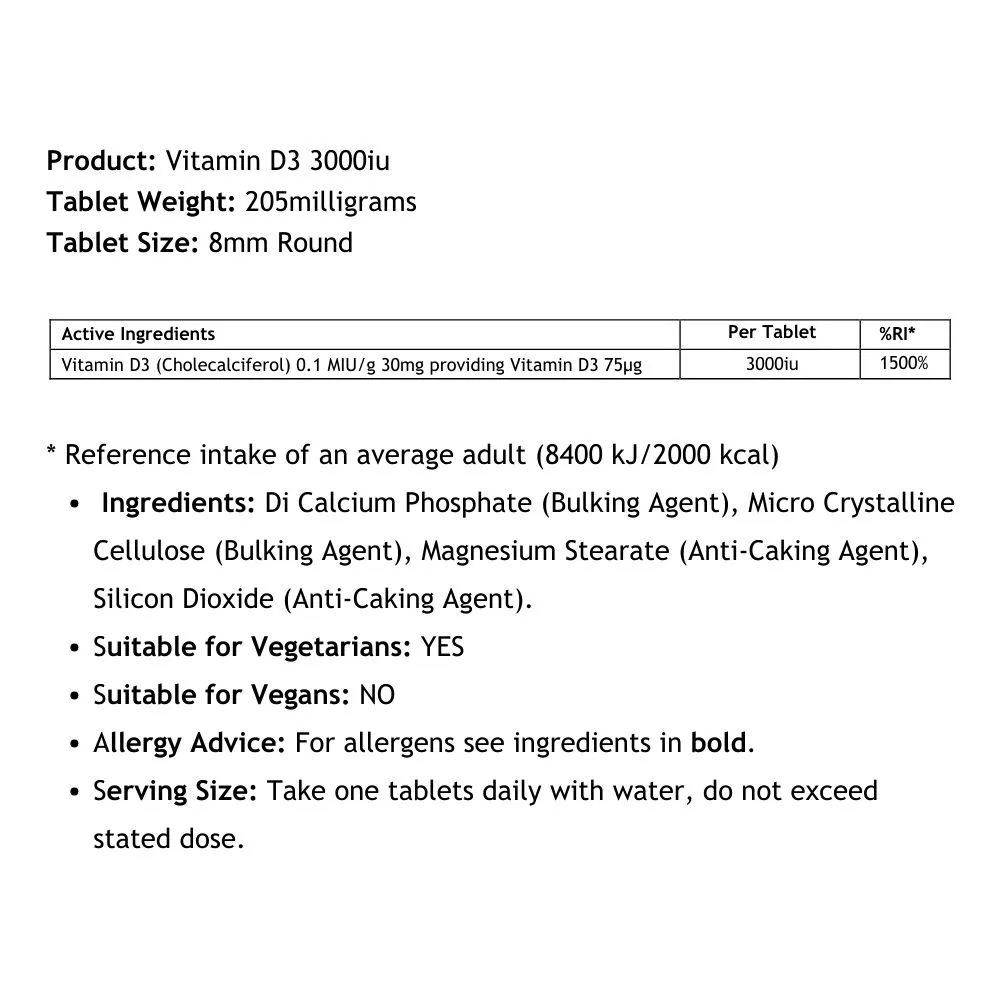
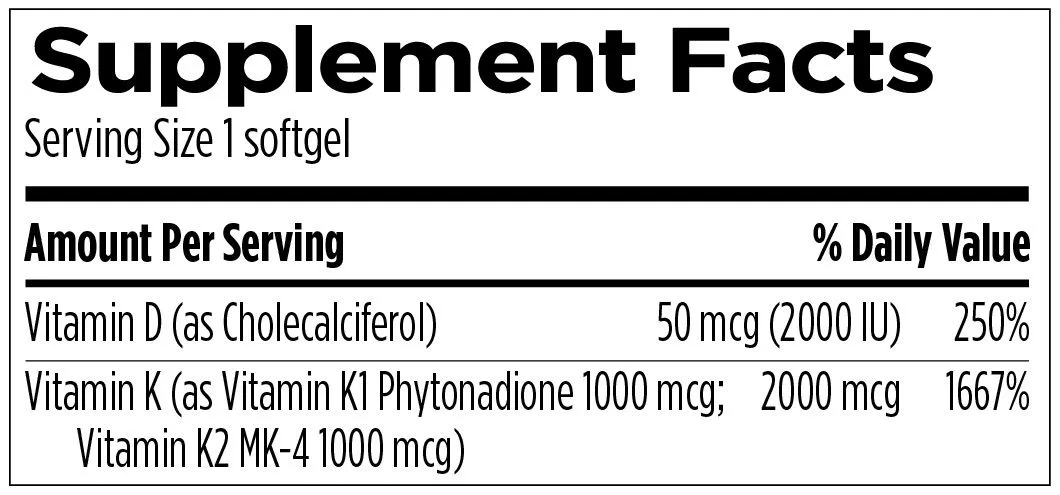
- Maintenance (Healthy Adults): 600–2,000 IU/day.
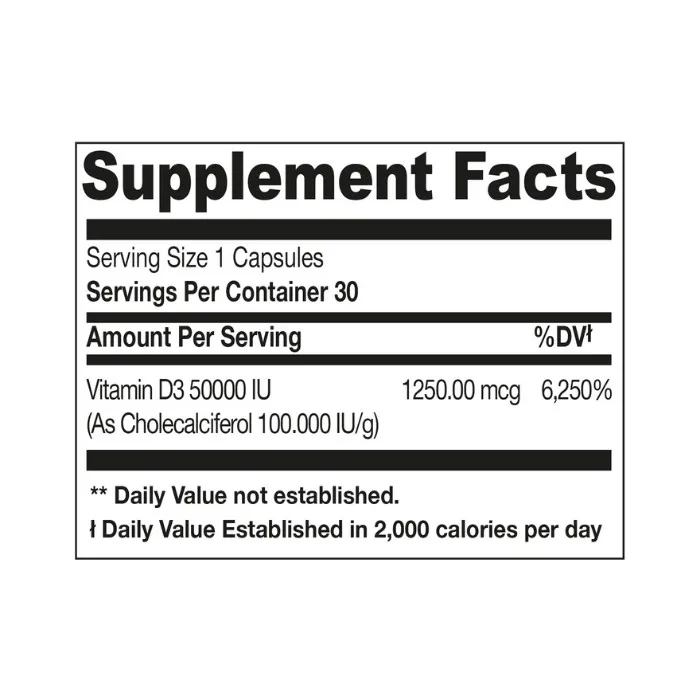
- Deficiency Correction: 50,000 IU weekly for 8–12 weeks, followed by maintenance.
- Special Populations: Patients with malabsorption syndromes (e.g., Celiac, Crohn’s) or those on anticonvulsants may require significantly higher doses (up to 10,000 IU/day).
Risks, Side Effects, and Contraindications
While Vitamin D3 is generally safe, excessive intake leads to hypercalcemia, which can be life-threatening.
Potential Side Effects
- Hypercalcemia Symptoms: Nausea, vomiting, constipation, polyuria, polydipsia, and confusion.
- Long-term Risks: Nephrolithiasis (kidney stones) and vascular calcification resulting from prolonged hypercalciuria.
Contraindications
- Hypercalcemia: Absolute contraindication.
- Hypervitaminosis D: Elevated baseline levels.
- Malabsorption Syndromes: Requires monitoring of fat-soluble vitamin absorption.
- Sarcoidosis/Granulomatous Diseases: These conditions may cause autonomous conversion of Vitamin D, increasing the risk of hypercalcemia.
Drug Interactions
| Drug Class | Interaction Effect |
|---|---|
| Thiazide Diuretics | May cause hypercalcemia due to decreased urinary calcium excretion. |
| Digoxin | Vitamin D-induced hypercalcemia can increase the risk of cardiac arrhythmias. |
| Orlistat | Inhibits absorption of fat-soluble vitamins (including D3). |
| Corticosteroids | May interfere with Vitamin D metabolism, potentially causing bone loss. |
Pregnancy and Lactation
Vitamin D3 is generally considered safe during pregnancy when taken at recommended doses. It is essential for fetal skeletal development. However, high-dose supplementation should only be conducted under strict medical supervision, as fetal sensitivity to Vitamin D can be unpredictable. Vitamin D is excreted in breast milk, but usually not in sufficient quantities to satisfy infant requirements; therefore, direct supplementation for the infant is often recommended by pediatricians.
Overdose Management
Toxicity is typically associated with chronic intake of >10,000 IU/day over long periods.
1. Immediate Action: Discontinue Vitamin D3 and calcium supplementation.
2. Hydration: Aggressive fluid resuscitation to promote renal calcium excretion.
3. Medication: Loop diuretics (e.g., furosemide) may be used to increase urinary calcium excretion.
4. Specialized Care: In severe cases, bisphosphonates or glucocorticoids may be required to inhibit bone resorption and lower serum calcium.
Frequently Asked Questions (FAQ)
1. How do I know if I am Vitamin D3 deficient?
Deficiency is diagnosed through a serum blood test measuring 25-hydroxyvitamin D levels. Levels below 20 ng/mL are generally considered deficient, while 20-30 ng/mL is considered insufficient.
2. Is Vitamin D2 the same as Vitamin D3?
No. Vitamin D3 (cholecalciferol) is the form naturally produced by human skin and is generally more effective at raising and maintaining serum 25(OH)D levels compared to Vitamin D2 (ergocalciferol).
3. Should I take Vitamin D3 with food?
Yes. Vitamin D3 is fat-soluble. Consuming it with a meal containing healthy fats significantly improves intestinal absorption.
4. Can I get enough Vitamin D3 from the sun?
While possible, it is inconsistent due to factors like latitude, time of day, skin pigmentation, sunscreen use, and age. Oral supplementation is the most reliable method for maintaining therapeutic levels.
5. What is the upper limit of Vitamin D3?
The Institute of Medicine (IOM) sets the Tolerable Upper Intake Level (UL) at 4,000 IU/day for adults, though many clinical protocols safely utilize higher doses for short-term correction of deficiency.
6. Can Vitamin D3 help with muscle pain?
There is growing evidence that Vitamin D3 deficiency is associated with musculoskeletal pain and weakness. Correction often leads to improved functional outcomes in orthopedic patients.
7. Does Vitamin D3 interact with blood pressure medications?
Generally, no. However, patients on diuretics should be monitored for hypercalcemia, as these drugs can reduce calcium excretion.
8. How long does it take to see results from supplementation?
Serum levels usually begin to rise within a few weeks, but it may take 3 to 6 months of consistent supplementation to reach steady-state levels and realize clinical benefits on bone health.
9. Can I take too much Vitamin D3?
Yes. Excessive intake leads to toxicity (hypervitaminosis D), which causes hypercalcemia, potentially damaging the heart, kidneys, and blood vessels.
10. Does Vitamin D3 support the immune system?
Yes. Vitamin D3 plays a critical role in modulating both innate and adaptive immune responses, helping the body defend against pathogens and reducing systemic inflammation.
Disclaimer: This guide is for educational purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider or orthopedic surgeon before initiating or modifying any medication regimen.